Sridhar Venkatapuram, “Understanding the Challenges to Mass COVID-19 Vaccination: The Case of UK,” ORF Special Report No. 157, August 2021, Observer Research Foundation.
Introduction
Late evening on 20 November 2020, senior leaders of England’s National Health Service (NHS) received an email announcing that earlier that day a vaccine company had filed for emergency authorisation for the use of their COVID-19 vaccine. The aim of the email was twofold: to inform the NHS that an effective COVID-19 vaccine was likely in hand, and to instruct them that their organisations across the country should prepare to rapidly conduct the vaccine rollout. Less than two weeks later, on 8 December 2020, the UK initiated the world’s first mass immunisation programme against COVID-19, and the largest in the history of the NHS. Today the UK’s COVID-19 vaccination programme is considered amongst the most successful in the world. Over 75 percent of adults are double vaccinated, and close to 90 percent have received a first dose.[1]
The UK government then removed almost all COVID-19 restrictions in late July, despite strong warnings from scientists about the impending third wave of rising infections particularly due to the Delta variant. The government argued that the vaccination programme had broken the link between infections and deaths. Indeed, two weeks after the removal of restrictions, cases of infections and deaths were still dropping—surprising most experts within and outside the UK.[2]Despite recording one of the highest numbers of COVID-19 deaths in the world during the first waves, the UK’s vaccination programme appears to have largely brought the pandemic under control within its borders.
However, how long this protection will hold depends on several factors—both domestic and international. Domestic challenges include the percentage of people yet to be vaccinated—albeit small in number, these individuals have not been inoculated either due to their lack of easy access to a vaccine, or hesitancy. The unvaccinated could undermine the gains and add to the infection rate or, worse, the death count. Furthermore, underneath the impressive national aggregate numbers are important differences in vaccine uptake among different groups identified by age, ethnicity, and geography.
Internationally, a significant factor will be how the pandemic evolves outside the UK borders, since the country remains vulnerable to potential new variants. Moreover, from an ethical and global access perspective, the UK securing more vaccines supply than is domestically needed and blocking the IP waiver at the WTO is seen as contributing to preventable COVID-19 deaths in many poor countries.[3]
This report describes some of the main facets of the UK COVID-19 vaccination programme. While much programme information is yet to be made public, details about its basic contours are publicly available.[a]The information included in this report has been gathered from official and public sources, as well as the author’s first-hand involvement with some policy and operations efforts related to the vaccination programme.
The UK Vaccination Programme: An Overview
Current Inoculation Coverage
According to official UK government data as of early August 2021, approximately 47 million first and 39 million second (i.e. close to 86 million total doses) injection doses have been given, and free of cost to individuals.[4]While the numbers are impressive, what also matters in an infectious disease pandemic is the location and percentage of the population that have been vaccinated. Some 88.7 percent of all UK adults (18+) have received a first dose, and 73.5 percent have also received their second dose. This is amongst the highest uptake of a COVID-19 vaccine by a national population anywhere in the world. It shows effective institutional mobilisation and delivery infrastructure as well as a culture of compliance and the people’s trust in public health institutions.
Starting with a few hundred or thousand injections per day in December 2020, the UK programme quickly ramped up by January 2021, delivering over 150,000 doses per day across the country. This was possible because vaccines were ready in vials well before they were authorised.[6]Vaccinations were first given to high-risk groups, including healthcare workers, residents of care-homes, clinically vulnerable people, and the elderly.[7]Thereafter, the programme distributed vaccines to the general UK population by age group, in five-year age bands, starting with the oldest; by mid-June, vaccinations were available to everyone above the age of 18. The highest number of doses in one day were given on 20 March 2021, —around 750,000 first injections. By August 2021, the daily number of injections was down to 20,000–30,000 per day.
The impact of the vaccination programme on reducing infections and deaths has been significant. However, with the pandemic evolving due to new strains and mutations, more questions and challenges are arising: Who are the 10 percent of adults who are still unvaccinated in the UK, why have they remained so, and how can they be inoculated? Other issues relate to vaccinating young adults and children, and the potential if at all, of a third booster dose to prevent “breakthrough” infections and prevent milder forms of disease, and protect from new variants.
As of August 2021, four COVID-19 vaccines are currently being used in the UK: Pfizer-BioNTech (Pfizer); Oxford/AstraZeneca (AZ); USNIH-Moderna (Moderna); and Janssen/Johnson & Johnson (J&J). The Pfizer vaccine was the first to be approved by the UK Medicines and Healthcare Products Regulatory Agency (MHRA) on 2 December 2020, and the UK became the first country to do so.[9]It initially ordered 40 million doses in July 2020 and later another 60 million in mid-2021. For the AZ vaccine, developed at Oxford University and approved on 30 December 2020, the UK government ordered 100 million doses. It has now become the main vaccine of the UK programme.[10],[11]
The dominance of the AZ vaccine in the UK could be attributed to its relatively easier storage requirements. Unlike the Pfizer vaccine, which requires ultra-cold chain storage at –70 degrees Celsius, the AZ vaccine remains viable in regular fridge temperature (4 deg C or below). Other possible reasons for the preference towards the AZ vaccine may have to do with timing, initial investments in research, and the nationality of pharmaceutical companies.[b]As of May 2021, the UK government had also ordered millions of doses of four other vaccines (Novavax, GSK/Sanofi, Valneva, and CureVac) that are still in the research and development pipeline in various parts of the world.[12]
Figure 3: How the Vaccines Compare
Source:BBC News – The Visual and Data Journalism Team[13]
Organisations Involved
The rapid and successful rollout of vaccines in December 2020 was largely a result of the UK government’s actions taken in early 2020. First, it created the Vaccine Task Force (VTF) in April 2020, an idea credited to Sir Patrick Valance, the Chief Scientific Advisor.[14]Its mission is to “drive forward, expedite and co-ordinate efforts to ensure that the UK population would have access to a clinically safe and effective vaccine against COVID-19.”[15]The VTF was created within the Department for Business, Energy and Industrial Strategy (BEIS), with Kate Bingham, managing partner of SV Health Investments, a biotech private equity firm, serving as chair. This was an unprecedented decision—to appoint someone from the private sector, and without a salary, to the highest level of the civil service, at a time of national crisis. It could be attributed to the fact that high-risk biotech R&D investment expertise is largely held in the private sector, particularly in private equity firms. Moreover, equity investing professionals are likely to have the best relationships with the diverse vaccine companies and related industry players from small to large, both domestic and international. The membership of the VTF steering group was made public only in November 2020,[c],[16]and it was also revealed that the VTF had been given a ring-fenced budget with a clear and minimal approval process.[d]While the actual size of the initial budget has not been disclosed, a January 2021 government report on the UK’s vaccine delivery plan cited a total expenditure of £6 billion on purchasing vaccines, of which £2.9 billion was spent on buying doses.[17]The scale of the resources made available and the freedom the VTF was given were driven by the scale of economic and human costs.
In 2020, the pandemic was costing the UK economy approximately £20.8 billion per month in lost GDP.[18]Moreover, while no official government document states this as a motivation, for most of last year, the UK also had the second-highest number of deaths in the world from COVID-19, after the US.[19]With the belief that an effective vaccine would be the only true exit from the pandemic for the population—both in terms of preventing more deaths and rescuing its economy—the VTF became a crucial part of the government’s pandemic response.
A second important organisation involved in the UK Vaccine Programme is the Joint Committee on Vaccination and Immunisation (JCVI)[20]—a pre-existing group comprising scientific experts that advise government health departments across the four nations of the UK on immunisations and the prevention of infectious diseases. The JCVI reviews vaccine safety and efficacy, as well as the impact and cost-effectiveness of immunisation programmes. The Committee has the mandate to assess all data on diseases and vaccines and advise on the plans to get vaccines to the public. While the MHRA has regulatory functions regarding approvals, the JCVI appears to have the role of informing if and how to use particular vaccines in national programmes, such as when children should get which vaccines or which annual flu vaccines would be delivered and when. Based on this established role, the JCVI became the decision-making body on which COVID-19 vaccines to be used as well as the priority of the population groups. Perhaps the two most important decisions the JCVI made was to prioritise access to vaccines by age group, and to extend the time between the first and second doses to ensure that more people would be protected.
Issues in Procurement
A common pattern among the G7 countries that managed to initially acquire millions of COVID-19 vaccines was the preference for vaccines made in their own country. Since researchers and companies that were most likely to produce effective vaccines were domiciled in the G7 countries, governments pre-ordering vaccines were most likely to find them within their own countries or in others in the G7. However, in early 2020, trust levels were declining between even the richest nations, and the UK could not be sure that G7 allies would give them access to vaccines produced in their countries.
For instance, the US has the largest public and private science infrastructure for producing novel health technologies. Under the Trump administration, it was unwilling to provide PPE and ventilators to other nations, indicating the low likelihood of it providing easy access to newly developed COVID-19 vaccines to other countries, even allies. Consequently, “securing access” for rich countries, including the UK, meant not only placing orders with vaccine companies but also supporting and ensuring the domestic production of vaccines. Indeed, the US government invested in American companies; Germany invested in German companies; and the UK invested in the AZ vaccine. At the same, to spread its risk, the VTF ordered different vaccines from seven different suppliers, of which three (Pfizer, AZ, and Moderna) are now manufactured in the UK.[21]
Figure 4: Vaccines Portfolio in the UK
Source:“In graphics: the UK vaccine supply chain,” Financial Times[22]
In its 2020 end-of-year report,[e]the VTF states that the UK had secured a total of 357 million doses of different types and from different sources,[23]overcoming a number of challenges, including the high-risk nature of investing hundreds of millions into all parts of the vaccine research, development, and manufacturing pathway. A pivotal choice was made to deal directly with vaccine suppliers to ensure control over the procurement process. In early 2020 the UK was in a remarkably tough situation in relation to other countries.
The US seemed unlikely to easily supply vaccines to other countries and would likely leverage its potential vaccine supplies to influence foreign policy. At the same time, the UK, post-Brexit, was unlikely to be treated generously regarding vaccine allocations by EU politicians and policymakers. Therefore, the UK had to engage directly with the sources, researchers and vaccine companies. Being directly involved in creating an effective vaccine would allow it to produce and buy as much as it needed as well as use the capacity for other purposes, such as its own foreign policy agenda.
However, going to vaccine-makers directly posed yet another challenge: the UK would buy lesser amounts than other larger countries (e.g. the US) or consortium of countries (e.g. the EU or COVAX). Thus, to be attractive to suppliers who, in effect, had monopolies with limited supply, the VTF made creative deals to secure early supply. Kate Bingham clearly identifies this UK predicament but has not revealed details about the creative approaches. Creativity in some deals may have had to do with the prices paid, and others, with providing additional support in manufacturing and other regulatory processes. With respect to the AZ vaccine, considered a UK vaccine, the reason for its demand in countries outside the G7 is likely because the VTF/the UK government helped broker the deals (see Figure 7).
As vaccine candidates began to show promise in October and November of 2020, there was a sense of increasing competition among countries as well as with international organisations such as GAVI and its COVAX platform. While the initial rhetoric had been about solidarity amongst nations, national security paradigms quickly became the dominant framework. Moreover, with every nation trying to get vaccines to its people as early as possible, national medical regulatory agencies and processes gained importance. Anything to be used in the UK had to be approved by the MHRA. Responding to the unique situation, the MHRA is said to have dramatically changed their approach to evaluating vaccine applications, speeding up the process while maintaining scientific rigour.[24],[25]The three other vaccines ordered by the UK—Novavax, GSK, and Valneva—as well as vaccines produced by companies in China, India, Cuba, and Russia have not yet been approved.[26]
In addition to evaluating the potential use of new vaccines, the MHRA and JCVI continue to monitor previously approved vaccines for several reasons. First, medical trials do not usually involve millions of people, but some rare effects only become visible once a population of millions receive the medication or vaccine. Indeed, the AZ vaccine was shown to have a rare side effect of causing blood clots in young people, based on which the JCVI recommended that young people receive alternative vaccines. Second, since the main outcome of interest of the COVID-19 vaccine trials was the prevention of death, the approved vaccines were not studied to see if they also prevent serious illness or further transmission of infections. In this regard, some vaccines may perform better than others, which must be monitored and evaluated.
Distribution
One advantage the UK government had in vaccinating its population was provided by the NHS, under which every legal resident of the UK has need-based access to healthcare, provided free of cost at the point of delivery. Most individuals are registered at one of their local neighbourhood medical practices. A growing number of private clinics and hospitals cater to individuals with private health insurance as well as to international clients. However, the NHS remains the primary source of healthcare for UK residents and holds their contact and health information. This structure allowed for efficient mobilising for vaccine delivery, almost at the same time as investments were being made in mid-2020.
The NHS is also directly connected to the people most vulnerable to COVID-19. Older people are likely to have established links with a local GP given their ageing-related morbidities; those who live in long-term care homes, largely run by private companies, also have links with local hospitals as well as to the NHS and national public health bodies. Moreover, individuals with serious illnesses and impairments also have some relationship with the NHS and their local GP practitioners. Thus, the NHS had a fairly comprehensive register of the most vulnerable individuals and groups in the country, as well as a clear way of contacting them.
In the initial phase, all healthcare workers and the oldest and most clinically vulnerable individuals were offered vaccinations. For healthcare workers, inoculation was provided at their place of employment, since most of them were working during the lockdown. Vaccinations were also given in long-term care homes and to other older people in their homes. Finally, vaccinations were delivered in local GP practices, pharmacies, and mobile clinics in certain areas where infections were high. Once the rollout reached the general public, vaccinations were being offered in large stadiums.[f]
Ethical and Epidemiological Considerations
Social, political and personal ethics have been central to state response to the pandemic across the world as well as in the UK. A few issues are worth noting about the ethics of the UK’s vaccination programme under the larger COVID-19 response.
First, the UK government’s choice to deal directly with vaccine companies and ensure domestic manufacturing expresses a particular kind of political ethics regarding the duties of a government to its citizens. In the face of potential disadvantage to their own citizens in the global competition for life-saving vaccines, the government made available billions of pounds and tapped the best professionals in biotech equity investing to procure vaccines. However, this angle has not been addressed in the discussion on ethics. Most public discourse instead focus on the fair distribution of limited resources such as ventilators and ICU beds.
Second, in the context of a pandemic, with new vaccines being produced in limited supply, the JCVI had to decide the order or priority of who would get vaccines.[27]Since vaccinations aimed to prevent deaths, this essentially implied deliberating on whose deaths would be prevented first—this involved both epidemiological and ethical considerations. By December 2020, it was evident the highest incidences of deaths from COVID-19 were amongst older age groups and healthcare workers. The JCVI first rolled out vaccinations by professional role (healthcare workers), need/risk, and age. However, later records show that across all age groups and professions, the death rate was disproportionately higher for those from non-white communities.[28]The JCVI could have prioritised these minority communities, but chose instead to recommend vaccinations according to age groups for the general population.
Third, in considering the limited supply of vaccines, on 30 December 2020, the JCVI adjusted the rollout plan by increasing the time between the first and second doses.[29]This was based on an ethical judgement that more people being protected from death to a significant extent from one injection was better than fewer people being protected to a high extent from two doses. Moreover, some research showing that extending the gap between the first and second doses of the AZ vaccine provides even better immunity proved to be an enormously fortuitous aspect of the vaccine.
Key Challenges
A challenge for the vaccination programme, anticipated from the start of 2020, was vaccine hesitancy and refusal. Both globally and in the UK, there was visible public discourse propagating conspiracies regarding the pandemic, including possible nefarious intentions behind vaccinations.[30]Discussions were held within the NHS and the UK government about distrust amongst Black and Minority Ethnic (BAME) communities regarding government programmes and vaccinations. The VTF and its chair, Kate Bingham, shared similar concerns.[31]To address this, BAME communities were actively recruited to participate in vaccine trials to engage with them, and to mobilise BAME participants to become advocates for vaccinations within their communities.[32]
Figure 5: Take-Up amongst Ethnic Minorities
Source:BBC NewsThe Visual and Data Journalism Team[33]
While BAME communities were initially viewed as most likely to be vaccine hesitant, this possibly resulted from conflating barriers to access with hesitancy. This mistake became evident in the fact that BAME communities have easily taken up vaccinations, especially when efforts were implemented to reach these communities in their own neighbourhoods through trusted organisations. The groups that seem to truly be suspicious of the vaccinations have come as a surprise. One such group is healthcare workers, particularly nurses and other allied personnel.[34]Given their professional background, they feel justified in their skepticism of the safety of vaccines developed so quickly. They would rather skip the vaccine, as well as recommend others to do so in order to avoid the small chance of adverse effects or death.
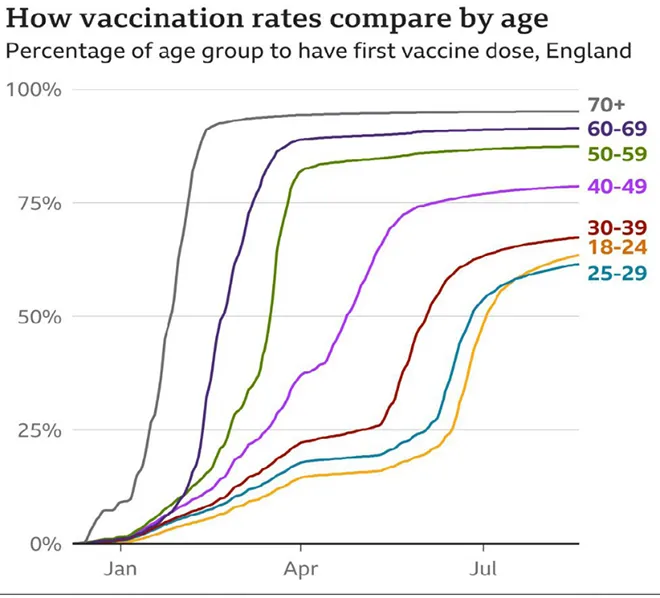
Another surprising group amongst the 10 percent of adults who remain unvaccinated despite being offered the opportunity are young people (20 to 30). There has been some research on the reasons,[35]and common ones are that the vaccines are seen to be unsafe—due to the speed at which the vaccines were developed, and that not enough time has passed since they were made available to reveal whether they have harmful side effects. Another reason is the belief that they are not at risk of getting the infection or dying from COVID-19; a result of much of the public discourse and media highlighting the lower death rates amongst the youth, despite being infected. Thus, many young individuals feel that the risks of harm from getting inoculated with new vaccines, especially ones that are using novel methods (RNA), may be higher than the risks of contracting COVID-19.
Figure 6: How Vaccination Rates Compare by Age & Region
Source:BBC News-The Visual and Data Journalism Team[36]
The government and public health bodies have implemented campaigns and outreach efforts to tackle the issue: monitoring which individuals are not vaccinated in healthcare settings; the increasing use of “vaccine passports” for entry to various venues, work and international travel; and making vaccinations more accessible. For example, in addition to walk-in appointments, vaccinations were also being offered at popular social venues such as nightclubs on weekend evenings.[37]
Global Access
Domestically, the UK vaccination programme has succeeded in containing deaths. In the context of an evolving pandemic, however, since much of the world’s people do not have access to COVID-19 vaccines while the UK is holding excess supplies, the success cannot be wholeheartedly affirmed. First, at a time when vaccine production and supply are limited, one country securing doses many times more than needed comes at the cost of other countries not having access to those vaccines. Even future supplies have been pre-ordered and secured by legal contracts by most of the wealthiest countries in the world. However, in the case of the UK, the VTF, while created primarily for the purpose of securing vaccines for the UK population, is also mandated to serve two other functions: to make provisions for the international distribution of the vaccines to the extent feasible;[38]and to create a long-term vaccine strategy to prepare the UK for future pandemics. The question then arises as to how the UK is dealing with the challenge of ensuring international distribution to overcome accusations of hoarding.
In August 2021, it was reported that the UK would likely possess 210 million excess doses of COVID-19 vaccines by the end of 2021.[39]These doses are not inclusive of the 467 million+ doses that are on order and still to be received by the UK. Even after vaccinating all citizens aged 16 years or above, as well as giving booster shots, the leftover vaccines purchased by the UK could protect more than 200 million people in the rest of the world. The UK government has announced that it plans on delivering 100 million of these doses to poor countries by June 2022, and has also provided funding for a billion vaccinations through COVAX. Presumably, the government is holding on to these vaccines and ordering more if it becomes necessary to inoculate children or to deliver a third booster dose.
Second, in terms of global access, the UK’s decision to block the temporary waiver of IP rights at the WTO is being perceived as siding with big pharmaceutical companies at the cost of public safety and health. Already, the US, France, Italy, and even China and Russia, have expressed their support for the WTO waiver. One reason for the UK’s resistance might have to do with the terms negotiated with vaccine companies early in 2020. Particularly interesting is the case of AstraZeneca, whose vaccine is by far the most ordered in the world outside of G7 countries; Bingham writes that the VTF/UK government helped broker many of those purchase agreements of the AZ vaccine, up to 3 billion doses by end of 2020.[40]
Figure 7: Global supply agreements of COVID-19 vaccines (doses/billions)
While the aggregate national statistics of vaccine coverage in the UK are impressive, there are troubling inequalities that require concerted effort to bridge. These differences are likely due to difficulties in accessing vaccines, vaccine hesitancy, or refusal. Minority communities, especially the BAME communities, must be provided increasingly better access. Furthermore, the relatively low vaccine uptake in London is of urgent concern, with a large population of young people remaining unvaccinated—this cohort could become the source of rising infections in the autumn and winter seasons. Greater effort is also required to distinguish between true “vaccine hesitancy” and “vaccine refusal” and implement different approaches to address both. For instance, health workers who refuse vaccinations might have legitimate concerns based on their expert understanding, which must be recognised, addressed and resolved.
Finally, in the international arena, the UK government can show leadership by clarifying the rationale behind its stockpiling of vaccines, and by highlighting its vaccine donations to low-income countries. The UK will improve its international reputation by supporting the IP waiver at the WTO. Such support does not preclude it from brokering more purchases of the AZ vaccine and will motivate more countries to develop vaccine manufacturing capacities for addressing future pandemics and ramping up overall health infrastructures.
Endnotes
[a]Some information may never be public including financial details, which are part of contractual terms with private companies, e.g. pharmaceutical companies, and are sealed or covered by non-disclosure agreements.
[b]In the US, Germany, France, Netherlands, Italy and others, the Pfizer vaccine is most popular, followed by the Moderna.
[c]This lack of transparency was the case with many of the groups the UK government set up in response to the pandemic.
[d]The VTF chair initially reported directly to the prime minister, and expenditure recommendations were made to a panel of four ministers for quick approvals.
[e]Published at the end of 2020, after six to seven months of operation.
[f]In the beginning, individuals were required to get an appointment for their vaccination. Once the programme evolved and the capacity to deliver increased, walk-in vaccinations were offered without appointments.
[1]“Vaccinations in United Kingdom,” Coronavirus (COVID-19) in the UK (COVID-19 Dashboard), The National Archives, 2021, https://coronavirus.data.gov.uk/details/vaccinations.
[2]Philip Ball, “Surprise dip in UK COVID cases baffles researchers,”Nature, 3 Aug, 2021, https://www.nature.com/articles/d41586-021-02125-1.
[3]Prabash Ranjan,The Case for Waiving Intellectual Property Protection for Covid-19 Vaccines, Observer Research Foundation (April 2021).
[4]Public Health England, “Vaccinations in United Kingdom.”
[5]“Cases in the United Kingdom,” Coronavirus (COVID-19) in the UK (COVID-19 Dashboard), 2021, https://coronavirus.data.gov.uk/details/cases.
[6]Department for Business Energy & Industrial Strategy,UK Vaccine Taskforce 2020. Achievements and Future Strategy(London, 2020), https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/944308/VTF_Interim_report_-_5th_publication.pdf.
[7] Department of Health & Social Care,UK COVID-19 vaccines delivery plan(London, 11 January 2021).
[8]Public Health England, “Cases in the United Kingdom.”
[9]Medicines and Healthcare products Regulatory Agency, “UK medicines regulator gives approval for first UK COVID-19 vaccine,” news release, 2020, https://www.gov.uk/government/news/uk-medicines-regulator-gives-approval-for-first-uk-covid-19-vaccine.
[10]Ian Bott and Clive Cookson, “In graphics: the UK vaccine supply chain,”Financial Times2021, https://www.ft.com/content/8b48a853-5b14-4378-91d4-17026fa15472.
[11]Department for Business Energy & Industrial Strategy,UK Vaccine Taskforce 2020. Achievements and Future Strategy.
[12]Department for Business Energy & Industrial Strategy,UK Vaccine Taskforce 2020. Achievements and Future Strategy.
[13]“Covid vaccine: How many people in the UK have been vaccinated so far?,” BBC News Services, 2021, https://www.bbc.co.uk/news/health-55274833.
[14]Kate Bingham, “The UK Government’s Vaccine Taskforce: strategy for protecting the UK and the world,”The Lancet397, no. 10268 (2021), https://doi.org/10.1016/s0140-6736(20)32175-9.
[15]Department for Business Energy & Industrial Strategy,UK Vaccine Taskforce 2020. Achievements and Future Strategy.
[16]Roger Highfield, “CORONAVIRUS: HOW THE UK BACKED VACCINE WINNERS,” (Science Museum Group, 2021). https://www.sciencemuseumgroup.org.uk/blog/coronavirus-how-the-uk-backed-vaccine-winners/.
[17]Department of Health & Social Care,UK COVID-19 vaccines delivery plan.
[18]Department for Business Energy & Industrial Strategy,UK Vaccine Taskforce 2020. Achievements and Future Strategy.
[19]“Coronavirus (COVID-19) Deaths,” Our World in Data, University of Oxford, Oxford Martin School, 2021, https://ourworldindata.org/covid-deaths.
[20]Blog Editor, “The roles of the MHRA and JCVI in COVID-19 vaccines,”Public Health Matters, 2 December, 2020, https://publichealthmatters.blog.gov.uk/2020/12/02/the-roles-of-the-mhra-and-jcvi-in-covid-19-vaccines/.
[21]Department for Business Energy & Industrial Strategy,UK Vaccine Taskforce 2020. Achievements and Future Strategy.
[22]Ian Bott and Clive Cookson, “In graphics: the UK vaccine supply chain,”Financial Times,(2021). https://www.ft.com/content/8b48a853-5b14-4378-91d4-17026fa15472.
[23]Department for Business Energy & Industrial Strategy,UK Vaccine Taskforce 2020. Achievements and Future Strategy.
[24]James Strachan, “COVID-19: Inside the UK’s Vaccine Taskforce,”The Medicine Maker, 14 July 2021, https://themedicinemaker.com/business-regulation/covid-19-inside-the-uks-vaccine-taskforce.
[25]Chris Kitching, Jane Kirby, and Ella Pickover, “UK ‘cut no corners’ when it approved Pfizer coronavirus jab, regulator says,”The Mirror, 2 Dec 2020, https://www.mirror.co.uk/news/uk-news/uk-cut-no-corners-approved-23103454.
[26]Thomas Ling, “COVID-19 vaccine UK: Everything you need to know about the new coronavirus jabs,”Science Focus2021, https://www.sciencefocus.com/news/covid-vaccine-uk/.
[27]Blog Editor The roles of the MHRA and JCVI in COVID-19 vaccines.
[28]K. Bhui, “Ethnic inequalities in health: The interplay of racism and COVID-19 in syndemics,”EClinicalMedicine36 (Jun 2021), https://doi.org/10.1016/j.eclinm.2021.100953, https://www.ncbi.nlm.nih.gov/pubmed/34169245.
[29]Chief Medical Officer Directorate,Coronavirus (COVID-19): vaccination guidance for health and social care professionals, Scottish Government (2021), https://www.gov.scot/publications/coronavirus-covid-19-vaccination-guidance-for-health-and-social-care-professionals/.
[30]Jill Lawless, “UK hits vaccine milestone, warns of ‘deadly’ misinformation,”AP News, 2 June 2021, https://apnews.com/article/europe-science-coronavirus-pandemic-coronavirus-vaccine-misinformation-3dd7ea21a88967aa3234e0cd3fabb631.
[31]Highfield, “CORONAVIRUS: HOW THE UK BACKED VACCINE WINNERS.”
[32]Department for Business Energy & Industrial Strategy,UK Vaccine Taskforce 2020. Achievements and Future Strategy.
[33]The Visual and Data Journalism Team – BBC News, “Covid vaccine: How many people in the UK have been vaccinated so far?.”
[34]Ian Sample, “Vaccine hesitancy in some health workers in England ‘may undermine rollout’,”The Guardian, 14 Feb 2021, https://www.theguardian.com/world/2021/feb/14/vaccine-rollout-caution-some-health-workers-england.
[35]Office of National Statistics,COVID-19 vaccine refusal, UK February to March 2021(7 May 2021).
[36]The Visual and Data Journalism Team – BBC News, “Covid vaccine: How many people in the UK have been vaccinated so far?.”
[37]NHS England and NHS Improvement London, “Heaven set to be first nightclub vaccination centre,” news release, 2021, https://www.england.nhs.uk/london/2021/08/06/heaven-set-to-be-first-nightclub-vaccination-centre/.
[38] Department for Business Energy & Industrial Strategy,UK Vaccine Taskforce 2020. Achievements and Future Strategy.
[39]Aubrey Allegretti, “UK set to ‘hoard’ up to 210m doses of Covid vaccine, research suggests,”The Guardian(London), 9 Aug 2021.
[40]Department for Business Energy & Industrial Strategy,UK Vaccine Taskforce 2020. Achievements and Future Strategy.
[41]Department for Business Energy & Industrial Strategy,UK Vaccine Taskforce 2020. Achievements and Future Strategy.
The views expressed above belong to the author(s). ORF research and analyses now available on Telegram! Click here to access our curated content — blogs, longforms and interviews.

 PDF Download
PDF Download

.png)










.png)
.png)